
A person living with inflammatory bowel disease may experience bile acid malabsorption which affects the gastrointestinal system and leads to physical and mental disturbances 1 2. Sadly, debilitating symptoms, such as urgency, watery stools, fecal incontinence, abdominal cramps, and fat-soluble vitamin deficiencies can occur and affects daily life activities1.
An academic paper published in 2020 establishes “Bile Acid absorption is altered in both pre-clinical models of Inflammatory Bowel Disease (IBD) and in human IBD.” 3 Therefore, understanding its essential role is crucial to develop research which innovates in the field contributing to better treatments and improves the quality of life of people living with this condition.

What is bile acid malabsorption?
Bile is more than a digestive fluid, as it plays a relevant role in gut health. This yellow-greenish liquid ensures your body absorbs fats and fat-soluble vitamins such as vitamin A, D, E, and K4. Additionally, it supports waste removal like excess cholesterol and bilirubin to maintain our body in balance along with playing a pivotal role in the composition of the gut microbiome by balancing bacteria in the small intestine5 6 7.
Bile can be classified into free, conjugated, primary and secondary bile acids. The liver produces primary bile acids while secondary bile acids are produced in the intestine through bacterial action on primary bile acids 7 8. Bile acid malabsorption occurs when the gut loses its ability to reabsorb bile salts, leading to an imbalance in digestive processes. As a result, these reach the colon instead of being recycled, disrupting bile’s essential functions1 9. When an excess of bile acids is produced or not properly absorbed it can cause diarrhea symptoms. This is also known as bile acid diarrhea 9.
Furthermore, bile acid malabsorption is not limited to patients with Crohn’s disease presenting ileitis or who have undergone ileal resection, since it can also present during clinical remission or in some cases in patients without ileal disease. This is due to bile acid metabolism deterioration10.
What are the diagnostics and treatments of bile acid malabsorption?
There are different tests used for the diagnosis of bile acid malabsorption, such as the SeHCAT (Selenium-75-homocholic acid taurine), the Serum C4 tests, and the Fecal BA test. The SeHCAT is the gold standard, even though it is not available in many countries. This test consists of swallowing a capsule with a low dose of a radioactive material (the tracer) and synthetic bile acid. Following the intake of the capsule, its components are absorbed in the small intestine and traced with a gamma camera on 2 different days, day 1 and day 7 1 10.
Discussing symptoms with your medical team is important to determine which treatment is appropriate, such as medical and/or dietary changes. Medical treatment consists of usually bile acid sequestrants that are known to work as a bile acid binder in the small bowel. Different types of medication include Colestyramine, Colesevelam, and colestipol 1.
Unfortunately, in clinical practice, bile acid malabsorption is a common but often overlooked and underestimated sign of inflammatory bowel disease10. This may lead to delayed diagnosis and patients not receiving the approriate treatment.
In what ways does bile acid malabsorption affect quality of life?
When I was diagnosed with inflammatory bowel disease, I had no knowledge of bile acid malabsorption. However, I began to notice a pattern: whenever I ate meals containing fats or oils, my urgency would be triggered. It was a frustrating process, not understanding why my body was reacting this way. Especially since I didn’t experience other typical inflammatory bowel disease symptoms like blood in the stool or abdominal pain. Another intriguing and crucial clue was my fecal calprotectin levels. I observed that whenever I experienced more bile acid malabsorption-related symptoms, my fecal calprotectin markers were elevated. I also suffered from extreme fatigue. Curious about how all of this could be connected, I began to explore more information.

The first time I learned that bile acid malabsorption might be related to persistent inflammation in inflammatory bowel disease was through an interview with Professor Dr. Mark Sundrud on the Propel a Cure for Crohn’s Disease website. In this research, it was astonishing to read, in a subset of patients, there may be a crucial link between bile acid malabsorption and inflammatory bowel disease. Through this research, I finally felt seen and validated that bile acids do matter. Simultaneously, connecting with other patients and hearing similar experiences led me to the insight that the role of bile acid malabsorption in inflammatory bowel disease may be more significant than we currently acknowledge.
That interview was life-changing for me. It encouraged me to take my symptoms more seriously and to actively seek treatment. Once I realized that my body was having difficulties absorping fats and oils, I knew I had to take action. The symptoms were debilitating and starting to limit my daily activities. I began with dietary changes, as this was something within reach, especially given the limited awareness of available medications at the time. Timely intervention turned out to be important.
Registered dietitian, Nicole Wake, sees in her practice the impact of bile acid malabsorption on patients and overall quality of life:
“Frequent watery diarrhea is the main symptom that I’ve seen in my clinical practice. Bloating and cramping are usually associated as well. Bile acid malabsorption leads to reduced absorption of nutrients which can lead to extreme fatigue and dehydration as well as weight loss or difficulty gaining weight. As far as quality of life I find my clients will be afraid to eat prior to having to go somewhere for fear of needing to go to the bathroom.”
How can nutrition help manage bile acid malabsorption and improve quality of life?
There are different dietary strategies currently recommended to manage bile acid malabsorption in inflammatory bowel disease;
“Dietary strategies for bile acid malabsorption include reducing intake of high-fat foods, consuming dietary fiber, but not too much. Fiber sources may need to be modified such as through soups or smoothies or being sure to cook vegetables well to improve tolerance in IBD. Eating small frequent meals rather than a large portion of food at once can reduce the pressure on the digestive tract and reduce bowel urgenc”, Nicole mentions.
Additionally,
“chewing foods well, eating slowly, and in a calm state are often techniques not highlighted enough but can have a significant impact on digestive function and reduce urgency and loose stools. Reducing the intake of high-fat foods and eating slowly and chewing well are strategies clients have highlighted as being most effective. Drinking fluids between meals can also help reduce the volume introduced to the digestive tract at one time and reduce bowel urgency”.
Although this study by McKenzie et al. was not specifically conducted among patients with inflammatory bowel disease and further research is needed, the findings suggest that food intolerances are common in patients with bile acid malabsorption. Diarrhea was most frequently reported after consuming take-away food, fish and chips, creamy sauces, cream, and large quantities of fruit. In contrast, foods such as potato, avocado, mango, watermelon, and pear were among the lowest frequencies to trigger symptoms. These findings partially reflect my own experience, as I tolerated foods like potatoes and watermelon quite well. In particular, boiled/steamed potatoes and carrots became an important part of my diet. Additionally, there are a few studies that suggest that certain foods, as well as cooking methods like steaming, may help bind bile acids in the digestive system and support their removal from the body through bowel movements. However, individual tolerances can vary significantly, so it’s important to consult with your dietitian before making any dietary changes.
Helpful resources about understanding and the management of bile acid diarrhea are BAD UK who is UK’s leading charity and provides a wealth of information and support to patients with bile acid diarrhea and Guts UK who also provides a downloadable printable guide.
What if our current understanding of inflammatory bowel disease is part of a bigger picture?
While the precise role and relationship of bile acids in inflammatory bowel disease remain under active research and have yet to be fully established, bile acids have captured the attention of researchers and are reshaping how we understand the disease:
- In an era where evidence-based medicine is the shape of a better future within the healthcare system, Quinn et al. took a bold step with their research paper published in 2020, “Global chemical effects of the microbiome include new bile-acid conjugations”.
This complex and very detailed study brought light to the scientific community, identifying phenylalanocholic acid (Phe-chol), tyrosocholic acid (Tyr-chol) and leucocholic acid (Leu-chol), by utilizing the Mass Spectrometry Search Tool (MASST), in 28 studies involving gastrointestinal samples from mice and humans. Per the research results, in the American Gut Project, these bile acids appeared in 1.6% of human fecal samples; being more frequently detected in patients with inflammatory bowel disease, cystic fibrosis and in infants compared to the general American Gut Project cohort.
These findings could reshape our current protocols and potentially add new biomarkers to be screened in patients with inflammatory bowel disase, specifically those presenting with bile acid malabsorption with bile acid diarrhea.
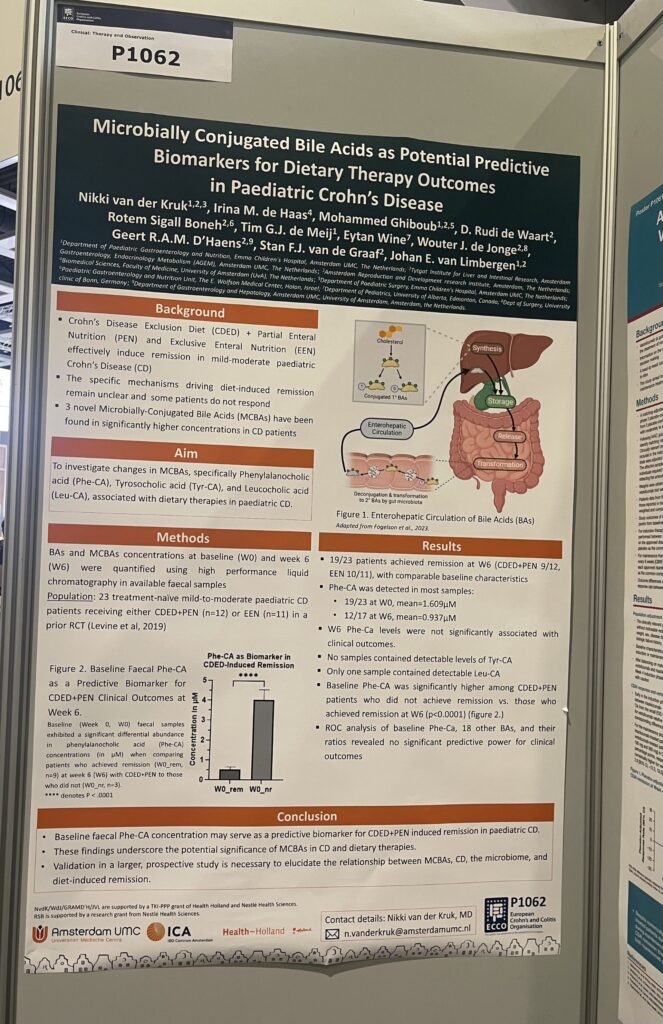
- “Microbially Conjugated Bile Acids as Potential Potential Predictive Biomarkers for Dietary Therapy Outcomes in Pediatric Crohn’s Disease” – Van Der Kruk et al. (2025)
After the outstanding findings by Quinn et al., another important research study has been conducted, bringing us closer to the use of microbially-conjugated bile acids (MCBAs) as potential biomarkers in patients with inflammatory bowel disease.
This study was performed in pediatric patients diagnosed with Crohn’s disease who followed dietary therapies Crohn’s Disease Exclusion Diet + Partial Enteral Nutrition or Exclusive Enteral Nutrition, which were evaluated in week 0(baseline) and week 6(outcome). They evaluated “(1) W6 remission vs. non-remission to identify if BAs were associated with clinical outcome at W6, and (2) baseline responders (achieving remission at W6) vs. non-responders to identify BAs predictive of W6 remission”. Using this they were able to determine the changes on the MCBAs of the patients at week 0 and week 6 and based on response (clinical remission was determined with PCDAI ≤10). The MCBAs used as markers were specifically Phenylalanocholic acid (Phe-CA), Tyrosocholic acid (Tyr-CA), and Leucocholic acid (Leu-CA), which are associated with dietary therapies in pediatric Crohn’s disease. They found that baseline fecal Phe-CA concentration might be a predictive biomarker for Crohn’s Disease Exclusion Diet + Partial Enteral Nutrition induced remission in pediatric Crohn’s disease.
- “The Impact of Confounders on Symptom–Endoscopic Discordances in Crohn’s Disease” Rajan et al. (2023) & “Association of Bile Acid Diarrhea with Symptoms and Disease Activity in Crohn’s Disease: Post-Hoc Clinical Trial Analysis of Serum 7a-hydroxy-4cholestern-3-one, C4, in Patients with Active Crohn’s Disease” – Battat et al. (2025)
Both these studies highlight that bile acid diarrhea may be a confounder, and the potential reason for the clinical symptoms and endoscopic inflammation discordance. - Farnesoid X recepter (FXR)
The Evans lab has researched the Farnesoid X receptor (FXR), a key protein that regulates the digestive system by sensing bile acids. FXR helps the body prepare for a meal by activating or deactivating various processes involved in digestion, blood sugar control, and fat metabolism. FexD may help restore balance in the gut, reducing inflammation without fully suppressing the immune system. It has only been used in animal models (preclinical research) so far.
Why do current research findings and treatments matter in clinical practice?
Ongoing research and growing recognition of the role of bile acids in inflammatory bowel disease are helping to drive new treatments forward. However, as noted before, in clinical practice, we still need greater awareness and decisive action from the moment of diagnosis. Patients need to be better informed about the possibility of bile acid malabsorption and current treatments. Another important consideration is that the long-term effects of bile acid malabsorption in patients with inflammatory bowel disease remain unknown. Therefore, it is essential to conduct further research to better understand its potential impact on disease progression and patient outcomes. In the meantime, it is crucial to continue utilizing available treatments to manage symptoms and improve patient quality of life. A referral to a registered dietitian is essential, as well as informing patients about available medications. If we collectively increase global and public awareness of bile acid malabsorption, we may improve the lives of many patients suffering from this condition timely. The role of bile acids in inflammatory bowel disease may open up a new, non-invasive avenue for treating gastrointestinal inflammation, which requires wider attention.
Thank you for reading. This article was provided free of charge to you. Since I learned about the potential role of bile acid malabsorption in inflammatory bowel disease through Propel a Cure for Crohn’s Disease informative research library, I’m dedicating this article to their outstanding work. If you have found the information in this article to be helpful, it is highly appreciated if you would please consider donating to them. Propel a Cure for Crohn’s Disease is a goal-oriented nonprofit organization raising funds for innnovative research aimed at identifying the underlying cause of Crohn’s disease. Please click here to make a donation and read more about their groundbreaking mission and work here.
The medical content in this article is reviewed and written in collaboration with medical writer Cristal Román, MD.
The information in this article is for informational purposes only and is not intended as medical advice. Please consult with your healthcare provider before making any decisions regarding your health or treatment.
References
1. Bile acid malabsorption [Internet]. Cleveland Clinic. [cited 2025 Apr 7]. Available from: https://my.clevelandclinic.org/health/diseases/24312-bile-acid-malabsorption
2. Part A. Exploring How Those with Bile Acid Malabsorption (BAM) Experience their Wellbeing: An Interpretative Phenomenological Analysis using Photovoice Part B: Investigating the Relationship Between Bile Acid Malabsorption (BAM) and Quality of Life. Anxiety and Depression.
3. Fitzpatrick LR, Jenabzadeh P. IBD and bile acid absorption: Focus on pre-clinical and clinical observations. Front Physiol [Internet]. 2020;11:564. Available from: http://dx.doi.org/10.3389/fphys.2020.00564
4. Blanco A, Blanco G. Digestion – Absorption. In: Medical Biochemistry. Elsevier; 2017. p. 251–73.
5. Chen I, Cassaro S. Physiology, bile acids. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2025.
6. Guzior DV, Quinn RA. Review: microbial transformations of human bile acids. Microbiome [Internet]. 2021;9(1):140. Available from: http://dx.doi.org/10.1186/s40168-021-01101-1
7. Di Ciaula A, Garruti G, Lunardi Baccetto R, Molina-Molina E, Bonfrate L, Wang DQ-H, et al. Bile acid physiology. Ann Hepatol [Internet]. 2017;16 Suppl 1(0):S4–14. Available from: http://dx.doi.org/10.5604/01.3001.0010.5493
8. Liu Y, Zhang S, Zhou W, Hu D, Xu H, Ji G. Secondary bile acids and tumorigenesis in colorectal cancer. Front Oncol [Internet]. 2022;12:813745. Available from: http://dx.doi.org/10.3389/fonc.2022.813745
9. Novel approaches to the diagnosis of bile acid diarrhea – Mayo Clinic [Internet]. Mayoclinic.org. [cited 2025 Apr 7]. Available from: https://www.mayoclinic.org/medical-professionals/digestive-diseases/news/novel-approaches-to-the-diagnosis-of-bile-acid-diarrhea/mqc-20479822
10. Vítek L. Bile acid malabsorption in inflammatory bowel disease. Inflamm Bowel Dis [Internet]. 2015;21(2):476–83. Available from: http://dx.doi.org/10.1097/MIB.0000000000000193